
Rib Fractures and Chest Wall Injuries From a Car Accident
Every breath is a reminder of the wreck. There is no cast for a broken rib, no quick fix. Just time, pain, and a paper trail the insurance company will try to pick apart.
On This Page
Rib fractures are the most common skeletal chest injury in motor vehicle crashes. Research published in Annals of Advances in Automotive Medicine identified rib fractures in 93.5 percent of severely or fatally injured seatbelt wearers. There is almost no treatment that speeds the bone along. Healing takes six to twelve weeks at minimum, pain often lasts months, and the imaging from those first weeks becomes one of the most compelling exhibits in the eventual claim.
What Actually Breaks Inside Your Chest
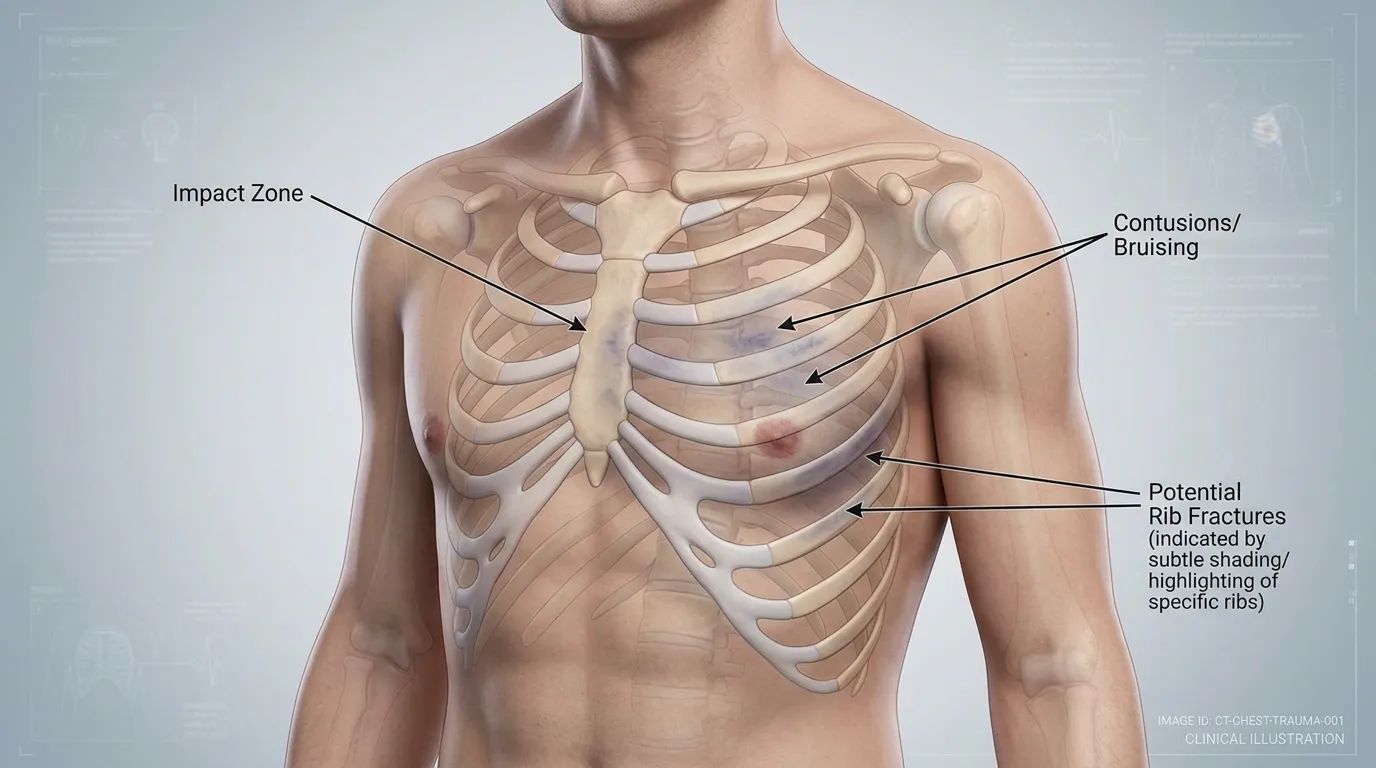
The chest wall is a cage of twelve pairs of ribs, a breastbone (sternum), the cartilage that connects them, and the intercostal muscles woven between every rib. Its job is to protect the heart, the lungs, the aorta, the liver, and the spleen while still flexing with every breath you take, somewhere between 17,000 and 25,000 times a day. Any forceful impact to the chest, whether from a shoulder belt, a steering wheel, a dashboard, an airbag, or a side door intruding into the cabin, loads that cage faster than it was built to flex.
What breaks first depends on age and impact angle. In younger occupants, the intercostal muscles and costal cartilage absorb some of the energy and the ribs themselves are springier. In older occupants the bone has less give, which is why the CDC reports motor vehicle crashes continue to kill an average of 36,791 Americans each year, with chest injuries over-represented in occupants 60 and older.
The injuries that travel with broken ribs
A rib fracture is rarely a problem unto itself. The danger is what the fractured rib does to the soft tissue inches away. A displaced rib end can puncture the pleura and collapse a lung (pneumothorax). It can tear the small arteries that run along the rib's underside and fill the chest cavity with blood (hemothorax). The impact that broke the rib can also bruise the lung itself, a condition called pulmonary contusion. An NHTSA Crash Injury Research and Engineering Network (CIREN) study found that 30 percent of pulmonary contusions in car crashes occur alongside rib fractures, and occupants older than 50 had nearly double the rate of rib fractures with pulmonary contusion compared to younger occupants.
How a Car Accident Breaks Ribs
Every crash rib fracture has a mechanism. Documenting that mechanism is one of the first things we do on these cases because it ties the bone to the event and forecloses the insurance argument that “the rib was already cracked.”

Shoulder belt loading
Seatbelts save lives. They also break ribs. In a frontal crash the shoulder belt locks, the torso decelerates against the webbing, and the force concentrates along a diagonal line from the shoulder to the opposite hip. Ribs 3 through 7, where the belt crosses, take most of the load. A study published in the International Journal of Legal Medicine reviewing 874 fatal crash cases found rib fractures in 685 of them, with restraint use not predictive of whether ribs fractured because belt wearers who died were in impacts severe enough to break ribs regardless. The broken ribs are the price of surviving a crash the belt helped you walk away from.
Airbag deployment

Frontal airbags inflate in roughly 30 milliseconds at speeds between 150 and 200 mph. That deployment saves lives in high-speed impacts, but the bag punches the chest wall hard enough to break ribs and the sternum on its own. A landmark study of post-mortem human surrogates published in Stapp Car Crash Journal isolated two distinct airbag loading phases, “punch-out” and “membrane,” and found that both produce rib fractures, with the combined effect producing more severe injuries than either phase alone. The bruising pattern from an airbag-loaded chest wall is distinctive enough that emergency physicians use it as a clinical marker for underlying sternal fractures, as documented in a case report in the Journal of Medical Case Reports where a visible airbag burn on the chest wall marked the exact location of a comminuted sternal fracture hidden on the initial X-ray.
Steering wheel and dashboard impact
Unbelted drivers and front-seat passengers without functional airbags take the steering wheel or dashboard directly in the chest. The impact crushes multiple consecutive ribs and often fractures the sternum as well. This is the classic “flail chest” injury pattern, where three or more consecutive ribs break in two or more places each, and a segment of the chest wall loses its connection to the rest of the ribcage. That flail segment moves paradoxically with respiration (inward on inhalation instead of outward), and breathing becomes mechanically impossible without ventilator support.
Side-impact and rollover crashes
In T-bone and rollover wrecks, the ribs on the struck side compress against the door panel. A 2019 review published in the IIHS fatality statistics continues to show that side-impact crashes remain among the deadliest per occupant, and crush fractures of the lateral ribs are one reason. These fractures tend to be displaced rather than hairline, and they are the ones most likely to puncture a lung.
Why There Is Almost No Treatment
Most broken bones get a cast. Ribs cannot be casted. Wrapping the chest tight was the old-school approach, but medicine abandoned it decades ago because it restricts breathing and increases pneumonia risk. The Mayo Clinic's trauma program explains that the typical healing time for a nondisplaced rib fracture in an otherwise healthy person is six to twelve weeks, and the treatment plan is limited to pain control, aggressive breathing exercises to prevent the lung from collapsing around the fracture, and activity modification.
Surgical rib fixation (called SSRF) exists, but it is reserved for severe cases: flail chest, multiple displaced fractures, or ribs that are not healing on their own after months. Most rib fracture patients are sent home from the ER with a prescription for pain medication, a spirometer to force deep breaths, and instructions to come back if they spike a fever or their breathing gets worse. The bone heals on its own, or it does not.
The treatment is time, and the insurance company knows it.
Because there is no surgery, no cast, and no dramatic rehabilitation protocol for most rib fractures, adjusters routinely argue the injury “was not serious.” That argument ignores the daily reality: sleep interrupted by pain every time you roll over, shallow breathing that invites pneumonia, lost weeks or months of work, and the radiology images that tell the real story.
The Symptoms That Bring People In
Rib fractures announce themselves. The pain is sharp, localized, and impossible to ignore. Here is the pattern we see in Kentucky crash clients almost every week.
Sharp pain with every breath
Inhaling expands the ribcage and pulls on the fracture. Patients describe it as “a knife” that stabs at the top of each breath.
Pain that worsens with coughing or sneezing
The sudden chest contraction against a broken rib is brutal. Many patients fear coughing for weeks.
Bruising along the seatbelt path
A deep purple line from the left shoulder to the right hip, sometimes with visible swelling over the broken ribs.
Tenderness to touch
Pressing lightly on the fracture reproduces the pain immediately. This is the single best bedside test.
Shallow, guarded breathing
Patients breathe in small sips to avoid expanding the ribcage. This raises pneumonia risk and should be treated.
Difficulty sleeping on the injured side
Lying on the fracture is unbearable. Many patients sleep in a recliner for weeks until the bone heals enough to tolerate a mattress.
Imaging That Shows the Damage
Rib imaging is where the case gets built. These are the studies that matter for both the medicine and the eventual claim.
- Chest X-ray (two views). The first study ordered in the ER. X-rays pick up most displaced rib fractures and rule out pneumothorax on the spot. They miss up to half of nondisplaced rib fractures, especially posterior ones.
- Dedicated rib series. Additional oblique views specifically angled to show the lateral ribs. Often ordered when the initial X-ray is clean but tenderness is significant.
- CT of the chest with thin cuts. The gold standard. A chest CT catches every fracture, shows pulmonary contusion, quantifies any pneumothorax or hemothorax, and excludes aortic injury. Every rib fracture patient over 50, and every patient with multiple fractures, should get one.
- 3D reconstructed rib imaging. Radiologists can now produce rotating 3D renderings of the ribcage from a chest CT. These images show every break in exquisite detail and are some of the most compelling exhibits a jury will ever see.
Radiology films are the exhibit that wins the case.
A chest CT or 3D rib reconstruction gives a juror something they can point to and count. Eight ribs. Two pneumothoraces. A sternal fracture. No amount of insurance-company hand-waving about “soft-tissue injuries” holds up against a rendered image of the client's own ribcage in pieces.
Complications That Change the Case
Most rib fractures heal without a complication worse than months of pain. The ones that do not heal cleanly have a few predictable paths, and each one meaningfully changes the settlement value.
Flail chest
Flail chest is the most lethal complication of a rib fracture. A 2023 study in BMC Anesthesiology reported a 19.9 percent mortality rate among flail chest patients, with 30-day mortality at 17.8 percent. Older patients with flail chest have mortality rates above 50 percent, and for patients over 80, a Consultant360 review of torso trauma in the elderly documented an 86 percent mortality rate. Survivors often spend weeks in intensive care on mechanical ventilation.
Pulmonary contusion
Bruising of the lung tissue itself. Shows up on CT as patchy ground-glass opacities, worsens for 48 to 72 hours after the crash, and can progress to acute respiratory distress syndrome. Pulmonary contusion is the leading thoracic soft-tissue injury in blunt chest trauma, and it accounts for a substantial share of ICU admissions after car crashes.
Pneumothorax and hemothorax
A collapsed lung (pneumothorax) or blood in the chest cavity (hemothorax) often requires a chest tube to decompress. Hospitalization runs several days. These complications are common enough that every multi-rib fracture should be watched for them in the first 48 hours.
Pneumonia
Shallow, guarded breathing because the fracture hurts leads to atelectasis (lung tissue that fails to fully expand), which in turn invites infection. Pneumonia occurs in 27 to 70 percent of flail chest patients who are not surgically treated, and when it develops, the mortality rate jumps to 51 percent. Even single-rib patients are at heightened pneumonia risk.
Chronic pain and disability
Clinicians have traditionally taught that rib fracture pain resolves in six to eight weeks. Research now shows otherwise. A prospective study of 203 rib-fracture patients at a Level 1 trauma center found that 59 percent still had prolonged chest-wall pain at two months, and 76 percent had prolonged disability. Among patients with isolated rib fractures, 64 percent still had pain and 66 percent still had work or functional limitations two months out. A follow-up study found that among isolated rib fracture patients, the prevalence of chronic pain was 28 percent and disability was 40 percent at six months. The traditional “you will be fine in six weeks” talking point is medical folklore, not evidence.
“I was one of those people who felt injury lawyers were not necessary if it was 100% the other party's fault. I was so wrong. They received over five times the amount initially offered and got the medical bills covered. Lesson learned. Insurance companies don't want to be reasonable anymore.”— Jill M., Kentucky client
Healing Timeline After a Kentucky Crash
No two rib fractures heal on the same schedule, but a few patterns are dependable.
| Stage | Timing | What Happens |
|---|---|---|
| Acute | Day 0 to 14 | Peak pain. ER evaluation, imaging, pain medication. Spirometer for deep-breathing exercises. Hospital admission if multiple fractures, pneumothorax, or patient over 65. |
| Early healing | Week 2 to 6 | Pain begins to ease, but every cough, sneeze, or sudden movement still hurts. Sleep disrupted. Most patients out of work or on light duty. |
| Late healing | Week 6 to 12 | Bone remodels. Pain fades to a dull ache. Patients return to desk work; manual labor still too painful for many. |
| Full bone healing | Month 3 to 6 | Final X-rays show a healed callus at the fracture site. Full clearance for physical work. |
| Chronic pain (if present) | Month 6+ | A meaningful share of patients have ongoing pain, stiffness, or disability well past the bone-healing point. This is where impairment ratings and future-care estimates come in. |
Kentucky Law on Rib Fracture and Chest Injury Claims
Two Kentucky statutes drive these cases.
No-fault and PIP. Under KRS 304.39-020, Kentucky is a choice no-fault state. Unless you formally rejected PIP in writing, the first $10,000 of medical bills after a crash are paid by your own auto carrier's PIP benefits. That covers ER visits, chest imaging, hospital admission, pain medication, and follow-up care. Most Kentucky drivers have PIP and do not know how to use it.
Statute of limitations. Under KRS 304.39-230, the deadline to file a motor vehicle injury claim in Kentucky is two years from the date of the last PIP benefit paid, not two years from the crash. Because rib fracture treatment often runs three to six months and chronic-pain follow-up can extend further, the effective deadline often stretches past the crash anniversary. It is still not a safe bet. Get the claim evaluated early so records are pulled before memories fade and adjusters lock down statements.
How Insurance Companies Undervalue Rib Fracture Cases
Rib fracture claims have a few standard attack patterns. Knowing them is half the battle. We don't let insurance companies minimize your pain, and here is what they typically try.
- “Ribs always heal.” Adjusters treat rib fractures as if they were a broken pinky. The chronic pain and disability research cited above says otherwise. A well-built claim presents the peer-reviewed literature alongside the client's own pain records, not generic assertions about how “most people are fine.”
- “There was no surgery, so it was not serious.” The absence of surgery is a feature of the injury, not a measure of how bad it was. Ribs cannot be casted and are rarely surgically fixed. That is a fact of thoracic medicine, not a reason to lowball.
- Minimizing imaging. Adjusters focus on an initial ER X-ray that showed “no acute findings” and ignore the follow-up CT that showed seven fractures. The full imaging record is what controls.
- Ignoring pulmonary contusion and pneumothorax. These are often scored separately in the medical record and have independent settlement value. Adjusters routinely bundle them under “rib fracture” for negotiation purposes. We unbundle them.
- Lowballing future care. Patients with chronic post-rib-fracture pain often need long-term pain management, nerve blocks, and physical therapy. Settlements that do not include future care leave the client paying out of pocket. Life care planners fix this.
- Arguing the crash was “too minor”. Low-speed collisions can still generate enough force to break ribs, especially in older occupants and belted drivers. The biomechanics literature is clear. Property damage photos do not determine the severity of an injury, and we have the medical witnesses to say so.
What Actually Drives Case Value in a Rib Fracture Claim
No two rib fracture cases settle for the same amount. Anyone posting dollar ranges online is guessing. What we can tell you is what moves the needle in the real-world negotiation, and what adjusters look at when they run their reserve numbers.
- Number and displacement of fractures on the CT. One nondisplaced rib reads differently than seven displaced ones on the same film. Radiology language like “displaced,” “comminuted,” or “multiple segments” is case value.
- Complications scored separately in the record. Pneumothorax, hemothorax, pulmonary contusion, and flail chest each carry independent weight. Adjusters try to bundle them under “rib fracture.” We keep them unbundled.
- Length of hospitalization and ICU time. ICU days, chest tube placement, and ventilator support all get reflected in the billing codes and medical narrative. Those records travel with the claim.
- Duration of documented pain. Research in the Journal of Trauma and Acute Care Surgery shows 59 percent of rib fracture patients still report pain at two months and 22 percent at six months. A pain journal and follow-up visit notes turn that statistic into evidence.
- Permanent impairment rating. A pulmonologist or physiatrist who assigns an AMA Guides impairment rating gives the claim a number that the insurance company has to account for.
- Age and pre-existing condition. Older occupants and patients with prior pulmonary disease have worse outcomes, which increases damages but also gives adjusters a pre-existing-condition argument to test.
- Wage loss and future care. Physical jobs, self-employment, and occupations that require lifting produce higher wage-loss claims. Future pain management, nerve blocks, and therapy go into a life care plan when the injury is chronic.
- Available coverage. Every claim is capped by the at-fault driver’s policy limits plus any uninsured or underinsured motorist coverage on the client’s side. A severe chest injury with minimum limits is still a minimum-limits case unless there is UIM.
We will not publish a dollar range. Every case is its own facts, its own imaging, its own coverage picture, and its own jury pool. What we will do is tell you, after we see the records, what the realistic settlement picture looks like for your specific case.
Bigger Share Guarantee®: You Always Get More.
Our clients always walk away with more than we do after all bills, liens, and costs are paid. Every case. No exceptions. If your share ever comes out less than ours, we cut our fee until it doesn't.
What To Do Next
If you are recovering from broken ribs or a chest wall injury after a Kentucky crash, here is the order of operations.
- Get full chest imaging. A plain chest X-ray is not enough if you have significant tenderness. Ask for a chest CT. If you are over 50, push harder. The CT finds fractures, pulmonary contusion, and any pneumothorax that a plain film misses.
- Treat the pain aggressively and use the spirometer. Pain control is not weakness, it is pneumonia prevention. Patients who breathe shallowly because it hurts invite infection. Use the incentive spirometer every hour while awake for the first two weeks.
- Keep every medical record. ER chart, CT report, discharge instructions, all follow-up visits, every prescription. The radiology images are especially important. Ask the hospital for the CT disc, not just the report.
- Document the pain day by day. A simple pain journal with daily entries is one of the most powerful pieces of evidence in a rib fracture case. Note sleep lost, activities avoided, and work missed.
- Do not give a recorded statement to the other driver's insurance. Adjusters ask questions designed to minimize the injury (“Can you take a deep breath?” “Are you walking around OK?”). Your answers get frozen into the claim file and used against you later.
- Use your PIP first. Kentucky law requires the other carrier to wait for PIP to pay through before bodily injury is owed. Proper PIP billing keeps medical bills from hitting collections and preserves the full bodily injury value.
- Call us. We evaluate rib fracture and chest wall cases at no cost and only get paid if we win. Tens of thousands of dollars in future care can be at stake if a complication develops, and early legal involvement protects both the medical record and the claim.
Related Resources From Sam Aguiar Injury Lawyers
Frequently Asked Questions
How long do broken ribs take to heal after a car accident?
Most nondisplaced rib fractures heal in six to twelve weeks. The Mayo Clinic reports that bone healing is usually complete within that window, but pain and functional limitation often extend well beyond it. Older patients, smokers, and those with multiple fractures heal more slowly.
Can a rib fracture be missed on the first X-ray?
Yes. Up to half of nondisplaced rib fractures are invisible on initial chest X-rays, especially posterior and lateral fractures. If tenderness persists past a week and the X-ray is negative, a chest CT usually finds the break. Do not let the ER “nothing acute” report end the investigation.
What is flail chest, and how serious is it?
Flail chest occurs when three or more consecutive ribs break in two or more places each. The disconnected segment moves paradoxically with breathing. Mortality ranges from 10 to 36 percent overall and climbs to 50 percent and higher in patients over 55. Most flail chest patients spend time on a ventilator in an ICU.
Why does my chest still hurt months after the crash?
Research published in PubMed found that 28 percent of isolated rib fracture patients still had chronic pain six months after injury, and 40 percent still had functional limitations. The old teaching that rib fracture pain resolves in six to eight weeks is not supported by the data.
Is an airbag supposed to break my ribs?
Airbags prevent fatal head and neck injuries but generate enough chest wall force to fracture ribs and the sternum in a meaningful share of deployments. A post-mortem biomechanics study confirmed both punch-out and membrane airbag loading produce rib fractures. Bruising or burning along the chest after deployment is a clinical marker for an underlying fracture.
How is a rib fracture case valued in Kentucky?
Case value turns on the imaging (number and displacement of fractures), complications scored separately in the record (pneumothorax, contusion, flail chest), hospital and ICU time, documented duration of pain, any permanent impairment rating, wage loss, and available insurance coverage. We will not publish a dollar range, because every case is its own facts. After we review your records, we can give you a realistic picture for your specific case.
Does Kentucky PIP cover chest imaging and hospital care?
Yes. Under KRS 304.39-020, Kentucky's no-fault PIP pays the first $10,000 of medical bills after a car accident, including the ER visit, chest X-ray, CT scan, and hospital admission. You must not have formally rejected PIP in writing for it to apply. Most Kentucky drivers have it.
Can I still file a claim if the crash looked minor on the outside?
Yes. Low-speed crashes can still generate enough force to break ribs, especially in older occupants and belted drivers where the shoulder belt concentrates load across the chest. Property damage photos are not a reliable measure of injury severity. Medical records and imaging are what controls.
What imaging should I ask for if I think I have a broken rib?
Start with a chest X-ray. If you have significant tenderness, a chest CT with thin cuts is the most accurate study. It catches every fracture, shows pulmonary contusion, and identifies pneumothorax or hemothorax. For older patients or multi-rib cases, a CT should be standard of care.
How soon should I call a lawyer after a rib fracture?
As soon as you are medically stable. Early involvement means pulling the crash report while evidence is fresh, preserving medical records before follow-up care fragments them, and keeping adjusters from locking you into a lowball statement. We evaluate rib fracture cases at no cost under our Bigger Share Guarantee®.